Skip to content
About Us
Our Team
Physical Therapy
Occupational Therapy
Speech Therapy
Developmental Disabilities Agency
Careers
Billing
Partners
Contact Us
About Us
Our Team
Physical Therapy
Occupational Therapy
Speech Therapy
Developmental Disabilities Agency
Careers
Billing
Partners
Contact Us
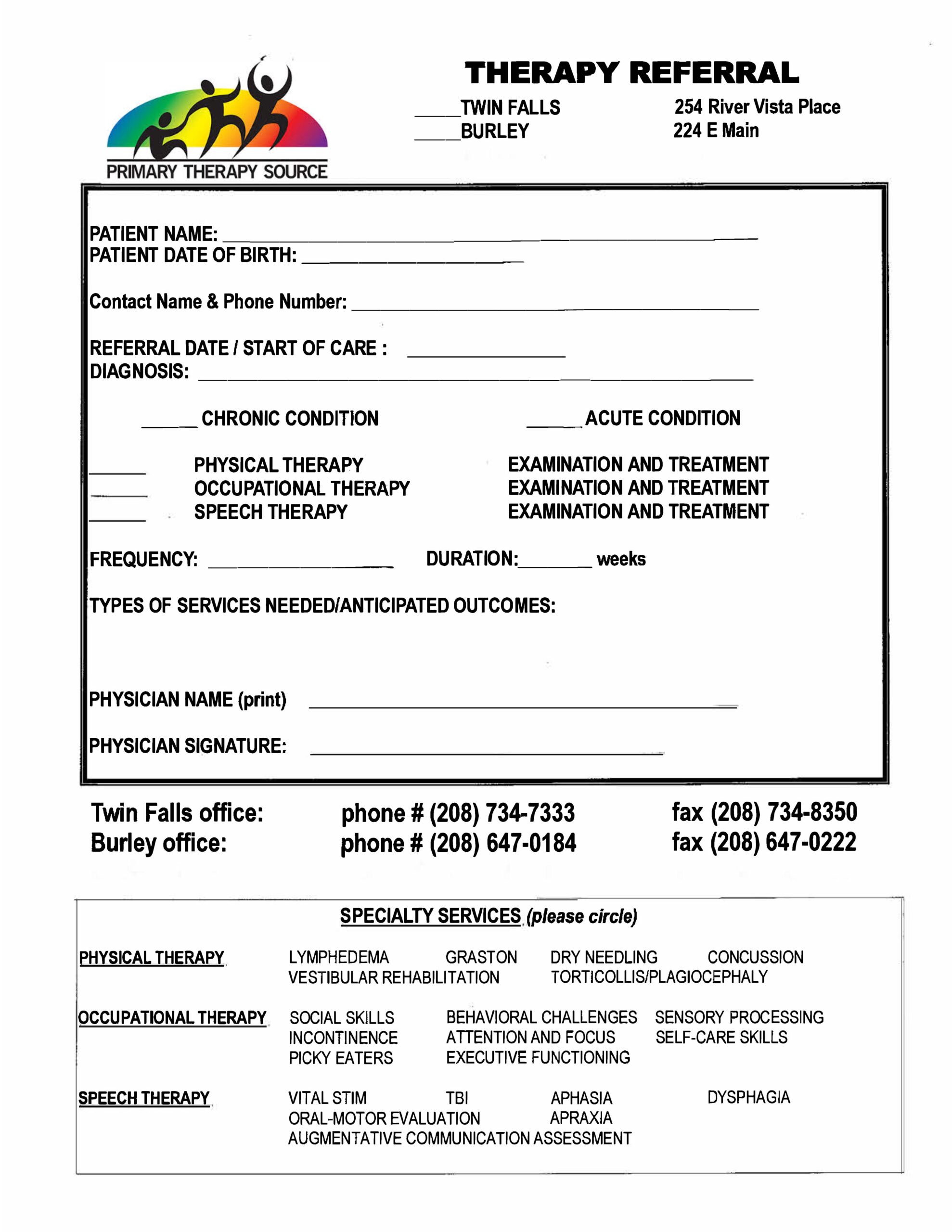
Physician’s Referral Form
Printable Form
Patient's First Name
Patient's Middle Name
Patient's Last Name
Date of Birth
REFERRAL DATE / START OF CARE :
DIAGNOSIS:
DIAGNOSIS TYPE
CHRONIC CONDITION
ACUTE CONDITION
Treatment Needed:
PHYSICAL THERAPY EXAMINATION AND TREATMENT
OCCUPATIONAL THERAPY EXAMINATION AND TREATMENT
SPEECH THERAPY EXAMINATION AND TREATMENT
FREQUENCY:
DURATION:
TYPES OF SERVICES NEEDED/ANTICIPATED OUTCOMES:
Physician's Name
Physicians Office Phone #
Send Referral